
Safety Alert: Fatal accident during lifting operations

In 2022 a RoRo vessel was in port for loading and unloading operations. Local stevedores and crew members were moving steel support beams that were part of the ship’s gear. During this work, a stevedore foreman was hit by sliding support beams and knocked over an edge to a lower deck. The beams fell on top of him.

The large shore crane normally used for the operation had been broken for several months and could not be used. A smaller shore crane was used, but this meant that the crane operator had limited lines of sight and could not see the guide cells on the deck into which containers were to be loaded. To improve crane operator lines of sight it was decided to move a stack of support beams that were stored on the aft deck on top of the housing of the ventilators. They were part of the ship’s gear and were occasionally used to transport 20ft containers.
The stevedore foreman and the duty officer decided to move the support beams one by one. A lifting plan had been made for this work two hours prior to the incident by the first mate and the stevedores’ foreman (who became the casualty). This had been agreed upon verbally and had not been put to paper.
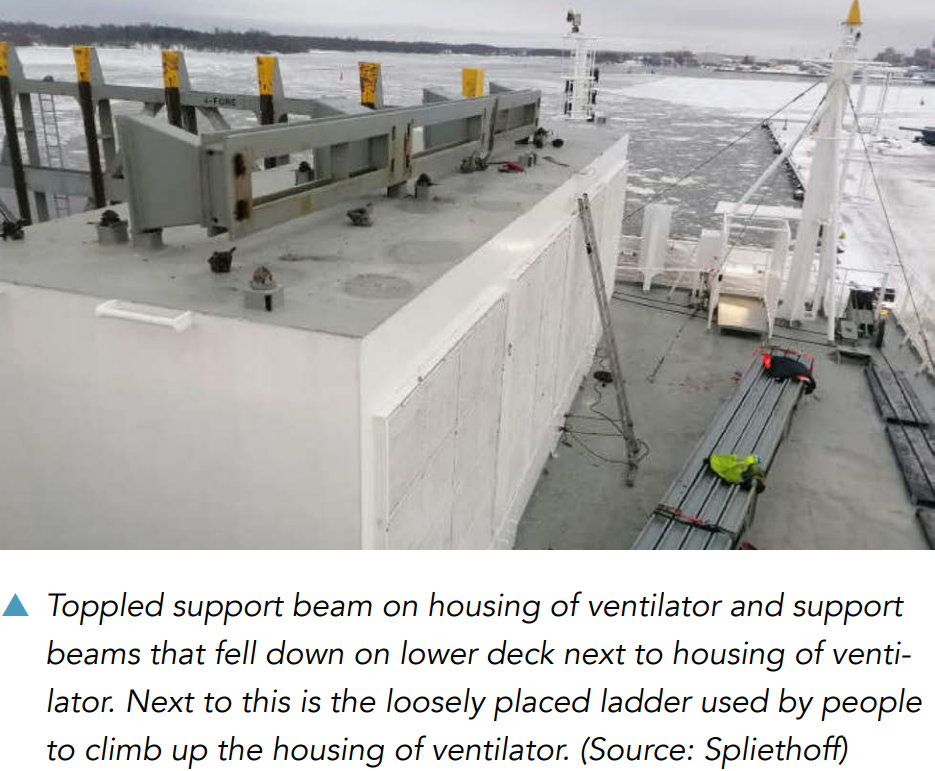
It was agreed that the stevedores’ equipment would be used, with the stevedores working together with the foreman, a signaller and the crane operator. On board, the foreman was assisted by the first mate and a cadet. They communicated in English. The stevedores communicated with each other in Finnish. During the operation, the first mate, foreman and cadet were standing on the raised deck of the housing of a ventilator, which they had climbed up using a loosely placed ladder. The support beams were to be hoisted ashore from this spot. The signaller was located elsewhere so as to provide the crane operator with instructions using gestures and radio.
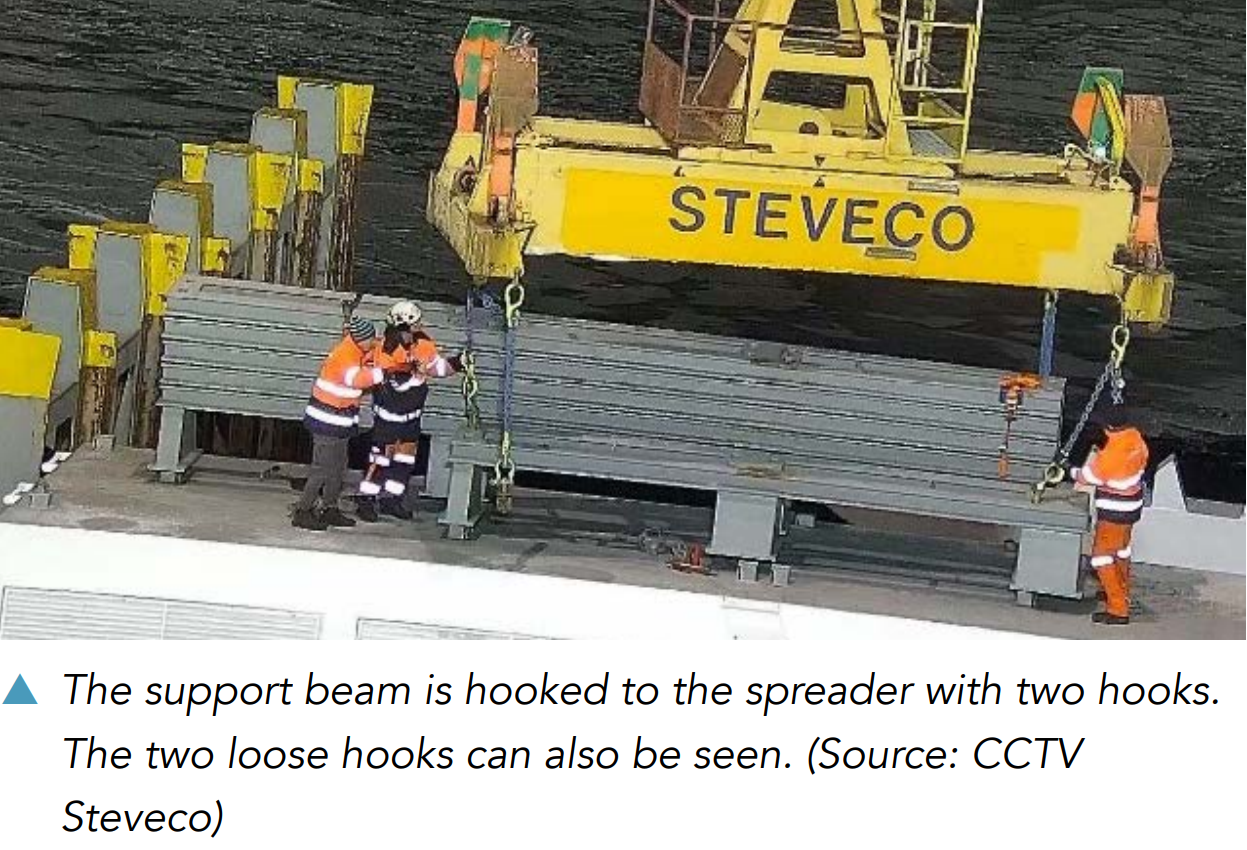
While hooking the support beams to the four corners of the spreader by chains and hooks, it became apparent that the hoisting height of the crane was insufficient. The foreman and the crane operator decided to shorten the chains. This was communicated to and coordinated with the first mate and the cadet. Shortened chains meant that only two chains from two corners of the spreader fit on the support beams. The other two chains were not tied up or secured; they remained loose. During the hoisting operations, the rear loose chain got caught on the stack of support beams. The beams, no longer secured by twistlocks, started sliding. They pushed the foreman off the housing of the ventilator, causing him to fall more than 2.5 metres onto a lower deck. The stack of beams then landed on top of him. The foreman suffered such serious injuries that they led to his death shortly afterwards.
Dutch Safety Board Investigative findings: Parts that were never used remained on the ship and obstructed the view. They were stored in a location that could not be easily reached and did not have a railing. The Lift Plan and Risk Assessment were not fit for purpose. Three people were in a dangerous location with no fall protection and no escape route close to a lifting load. After it became apparent that the initial lifting plan did not to work, a new plan and associated Risk Assessment were not undertaken. Loose chains remained attached to the spreader. Workers remained in the unsafe location without protection.
Lessons learned: review safe storage of equipment. After the accident, the operator decided to store the equipment on shore. Ad hoc work should always be risk assessed and planed, taking into account the need for a safe place of work. If at any point before or during the operation it becomes apparent that the work is not safe and/or practicable, a new risk assessed plan should be devised that clearly address safe working.
This material is from the Dutch Safety Board Shipping Occurrences Report January 2023 – July 2023 pages 13-14
CLICK HERE FOR THE FULL REPORT
ICHCA International is committed to helping industry to learn lessons fast, learn them once and make sure that they stay learnt. This information is intended to provide all organisations in the cargo supply chain with the opportunity to consider the events and to review and adapt their own health and safety control measures to proactively prevent future incidents.
We are grateful to Dutch Safety Board for providing details and for raising awareness. We acknowledge their commitment to sharing learning to benefit others. If you have similar operations, please share this information with managers, operatives and any potentially affected third parties as appropriate. Please also review any of your relevant operations for similar hazardous conditions, risks, and controls. Learning content like this is highly valuable as it is based on real-world experience. We encourage everyone with publishable information about incidents to send it to us, so that we can raise awareness across the whole industry. Please contact us at secretariat@ichca.com; sharing your insight could save a life or prevent injury.